Self-fulfilling prophecies: But is the prophet heard?
Seminar on Prediction Under Intervention(s), Leiden
2025-12-02
Prediction model performance versus healthcare impact
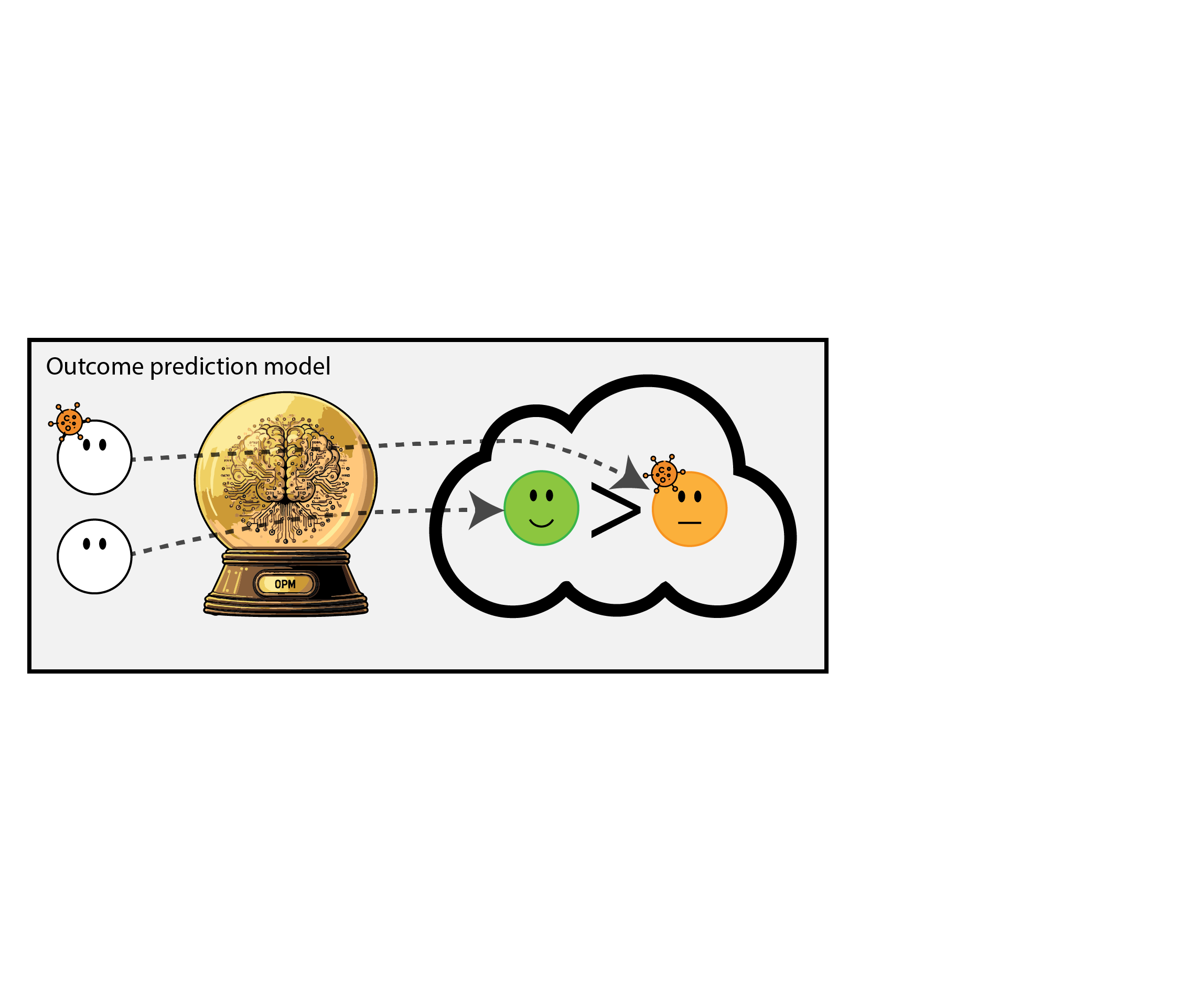
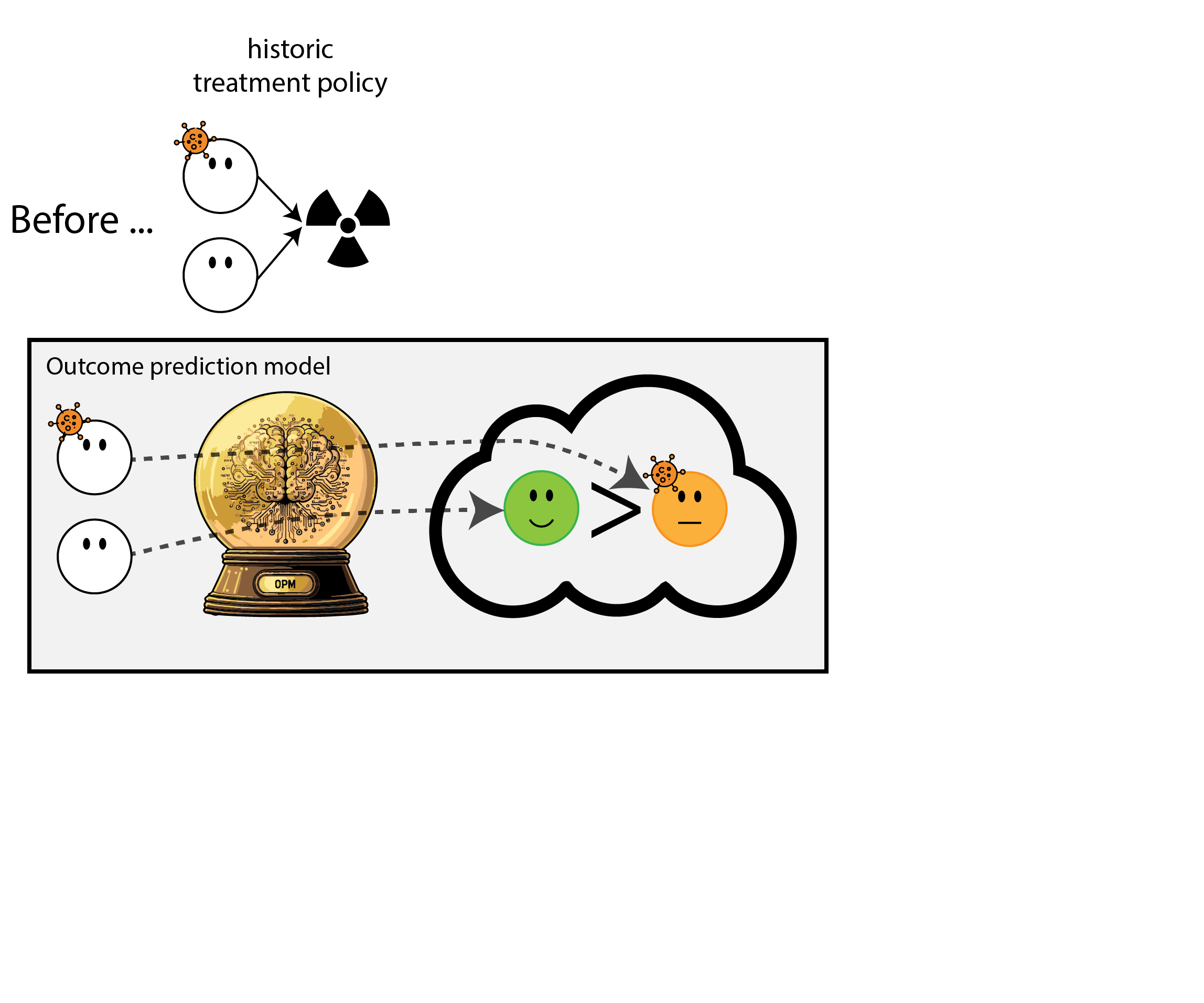
- many prediction models: given feature \(X\), estimate probability outcome \(Y\)
- e.g. given age, cholesterol and sex, predict 10-year risk of a heart attack
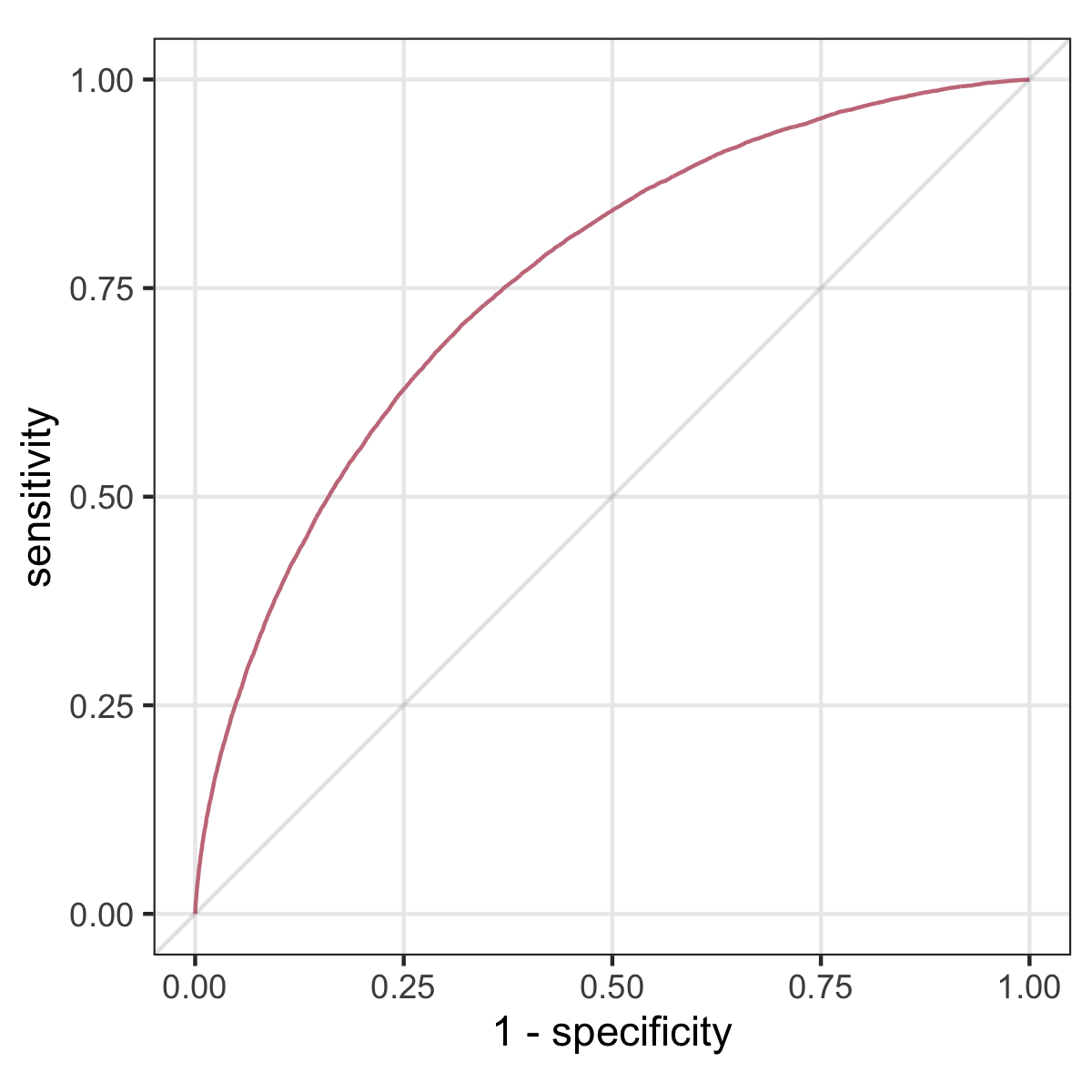
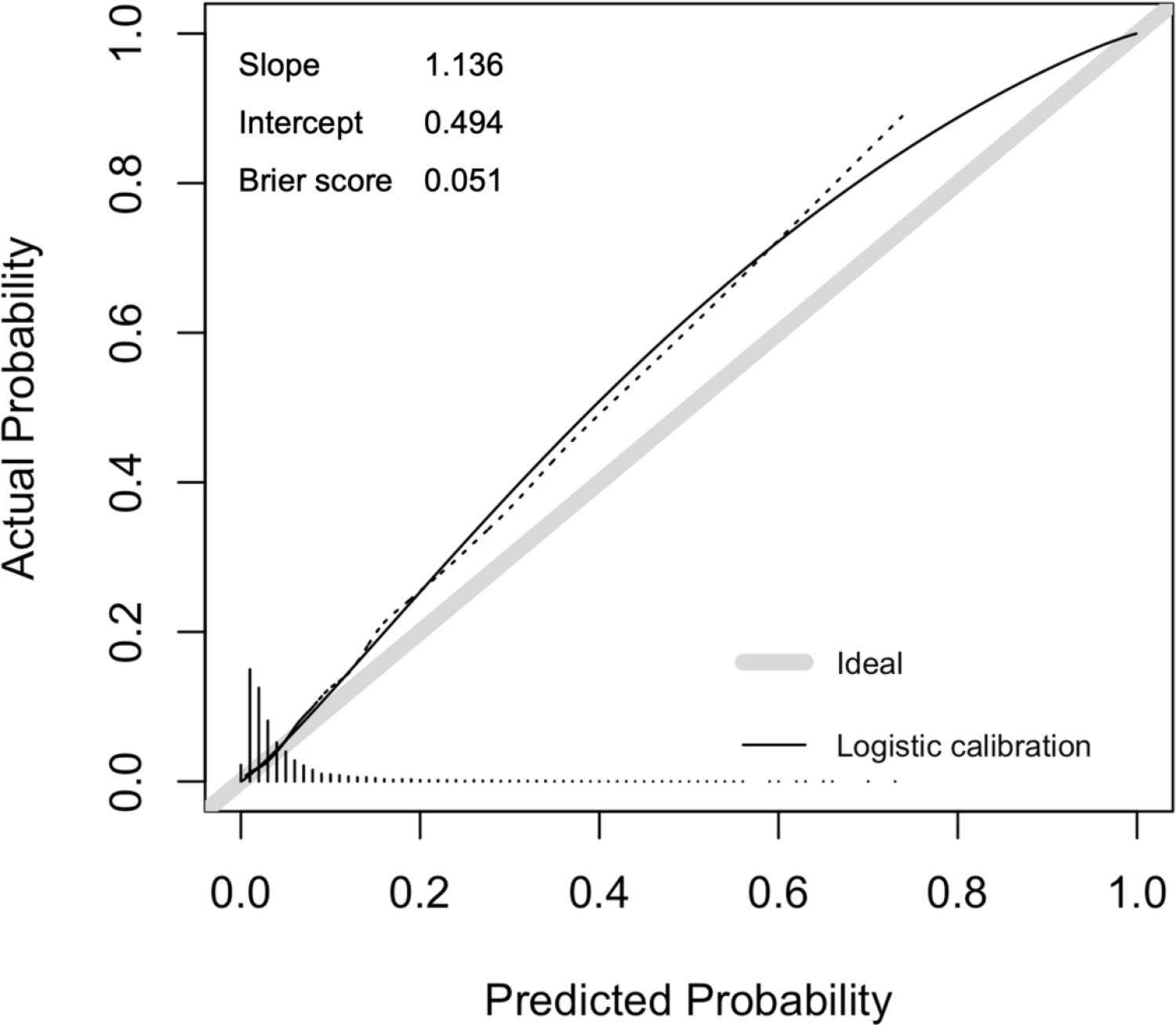
- evaluated on predictive performance: calibration and discrimination (AUC)
Regulation to the rescue: we need to monitor (AI) models
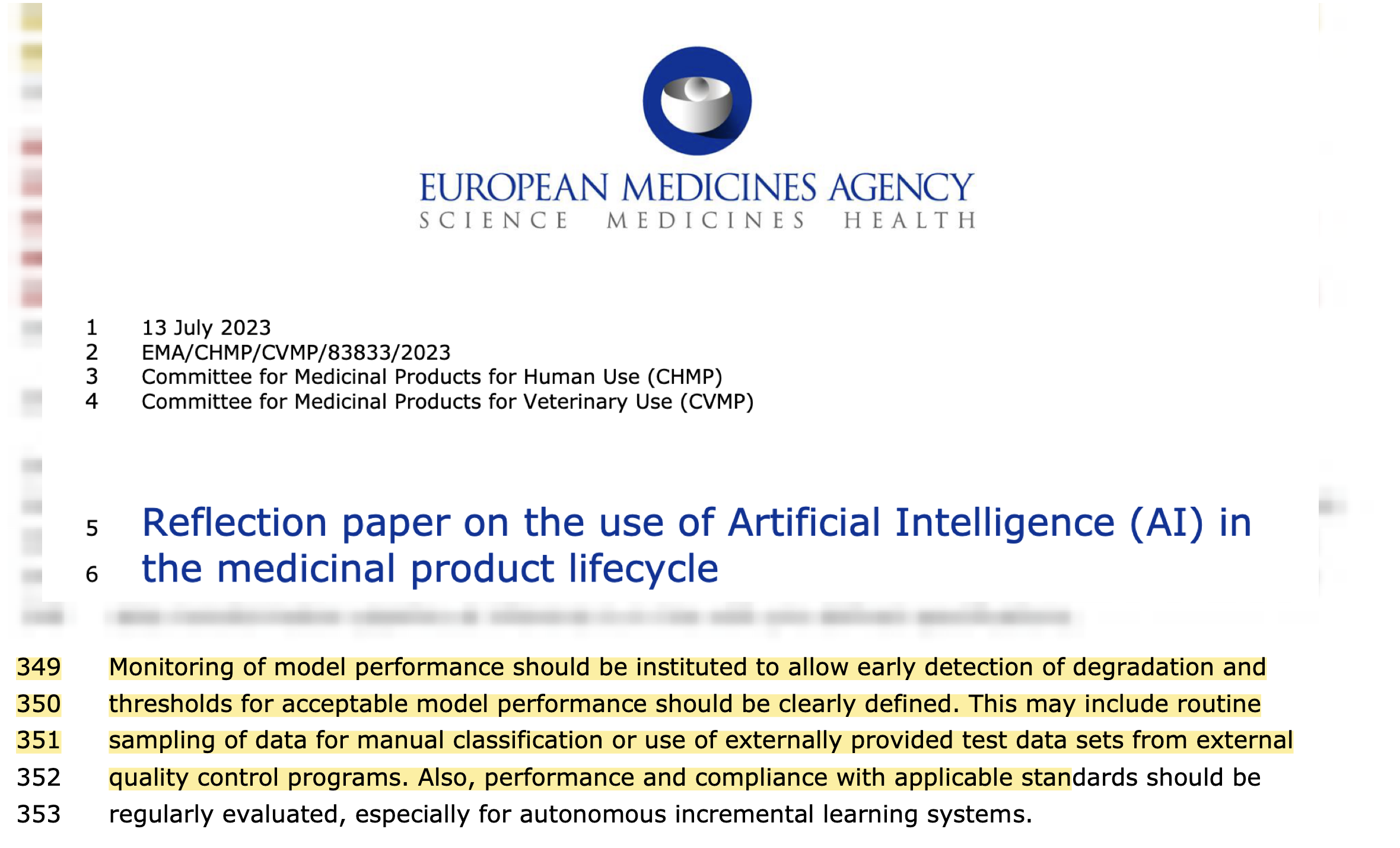
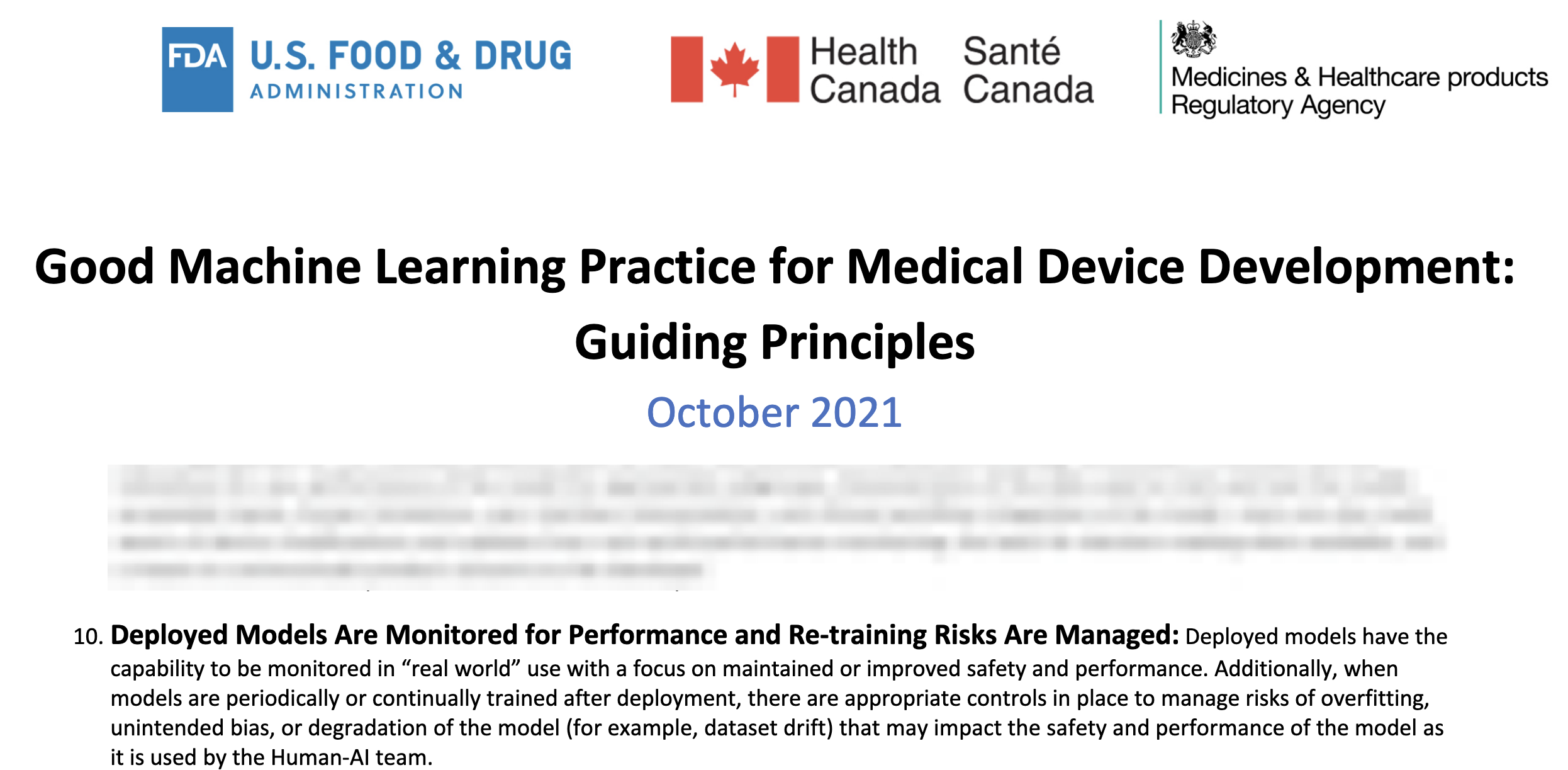
Let’s monitor the model performance over time
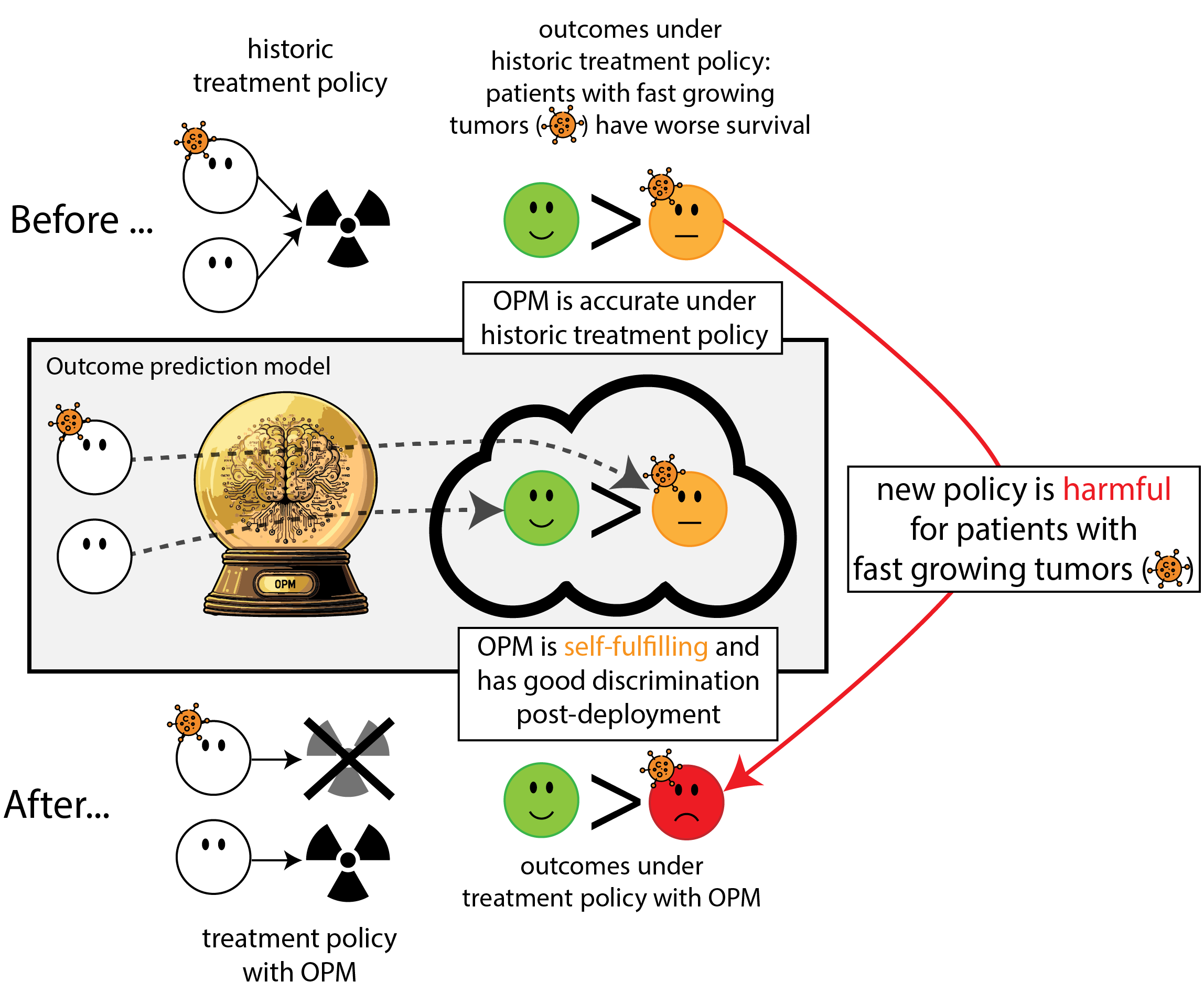
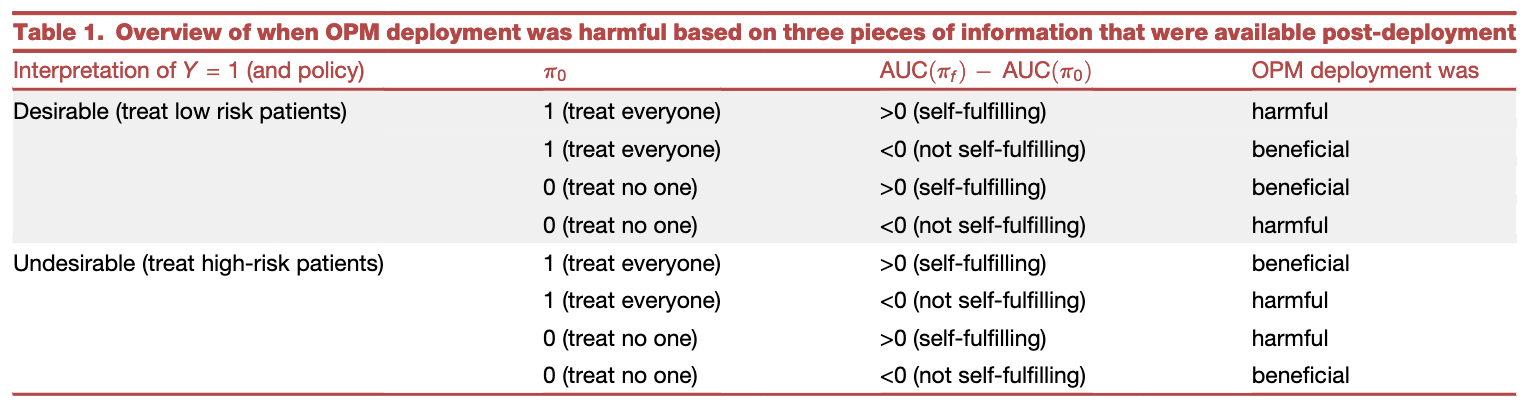
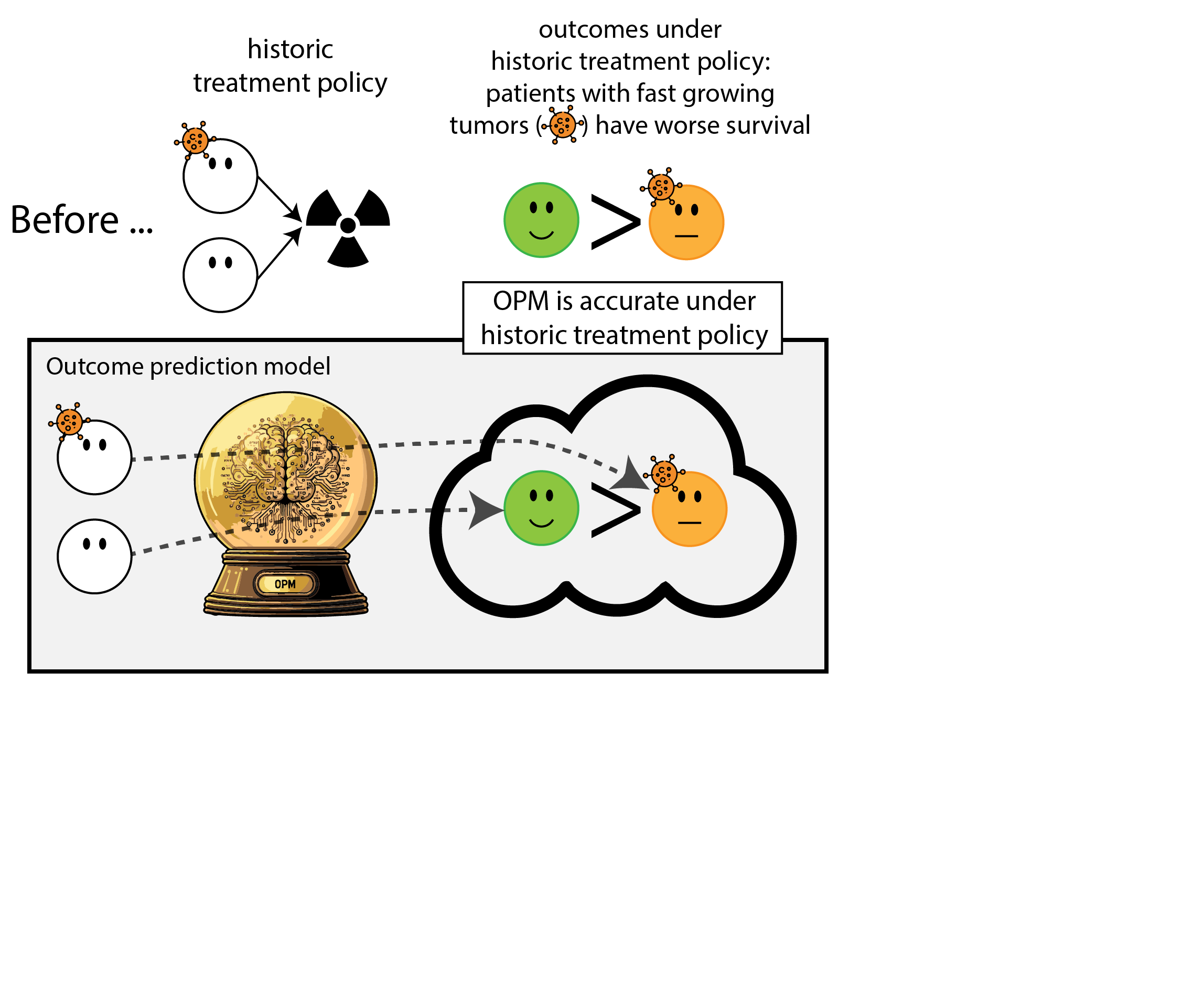
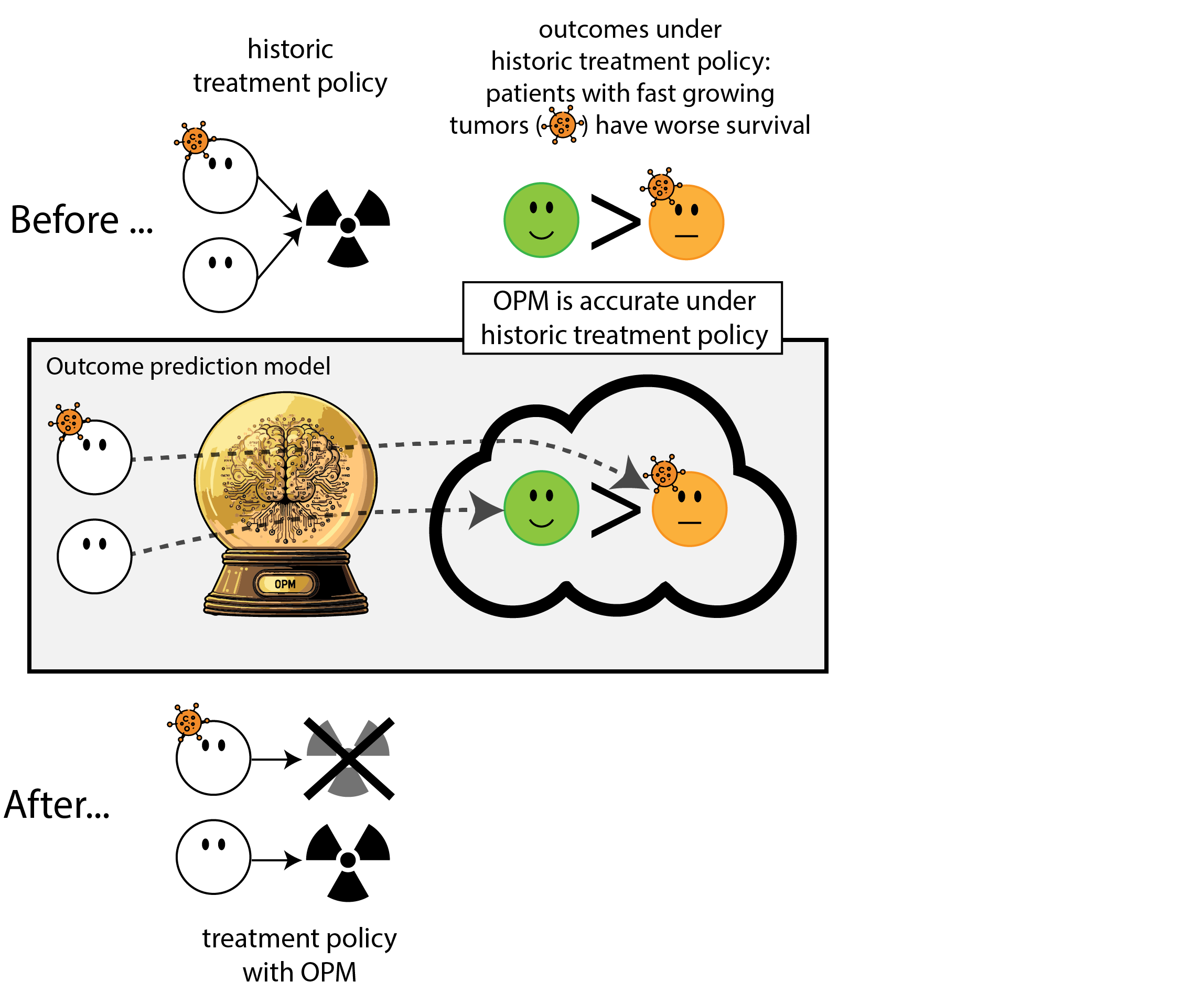
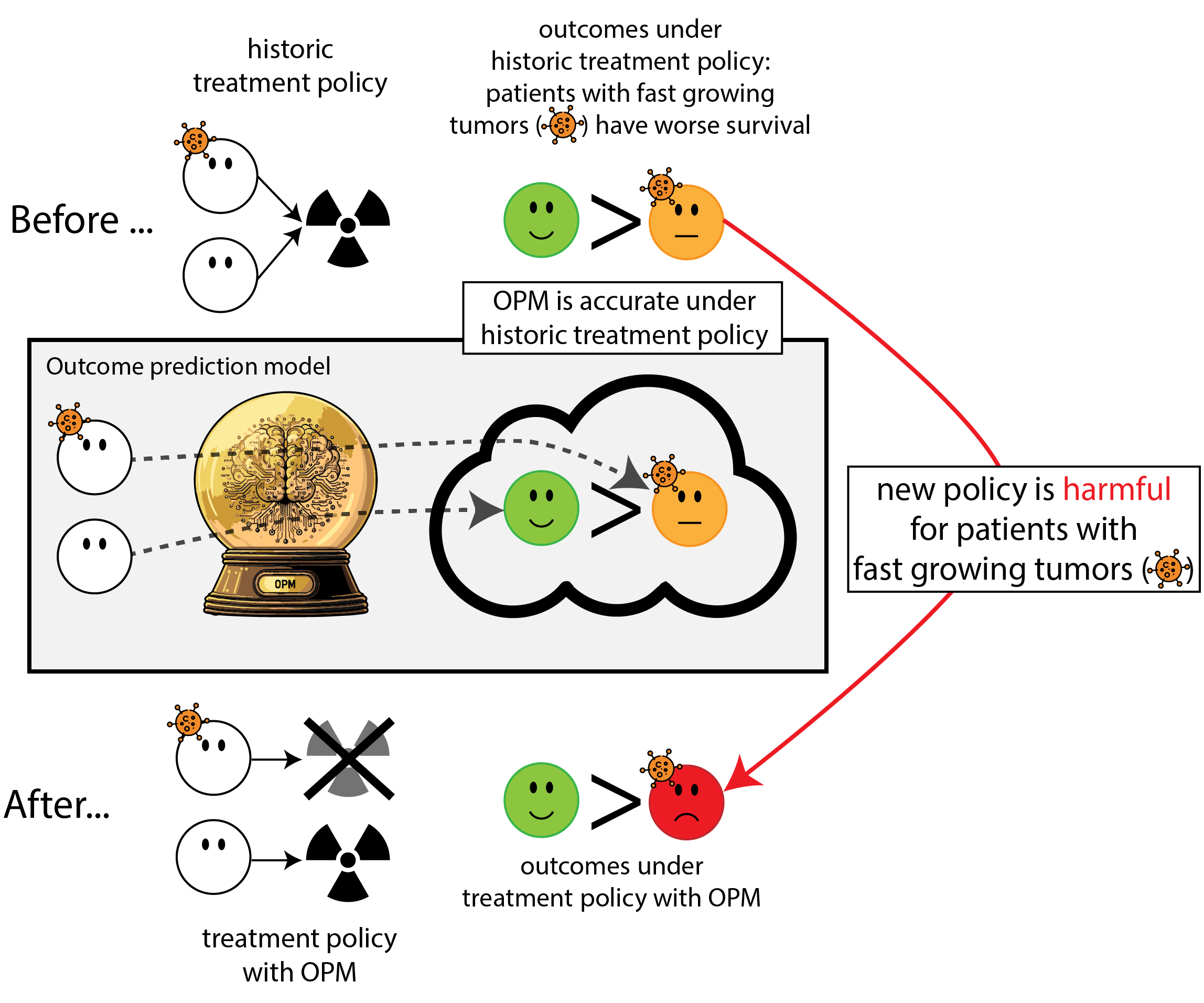
Harmful self-fulfilling prophecies occur in cases without extreme treatment (interaction) effects
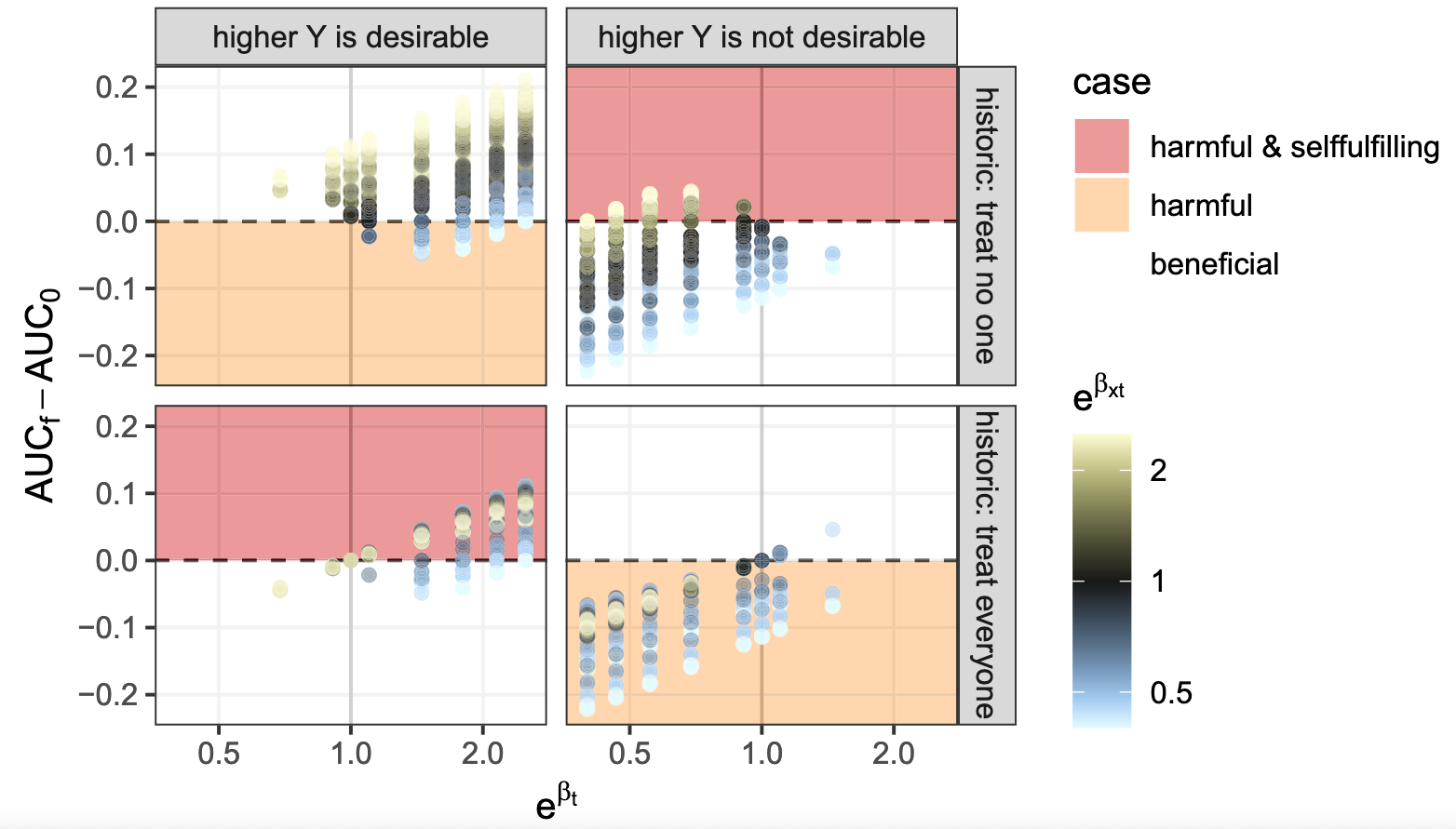
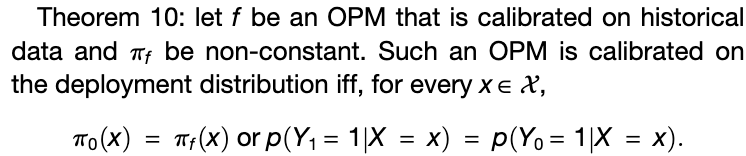
Calibration result

- ergo deployment of model was useless
Editorial


Press coverage - urgent mail
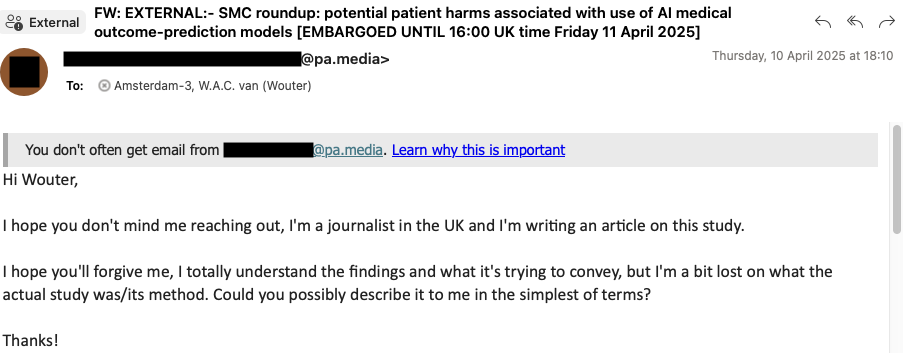
Press coverage
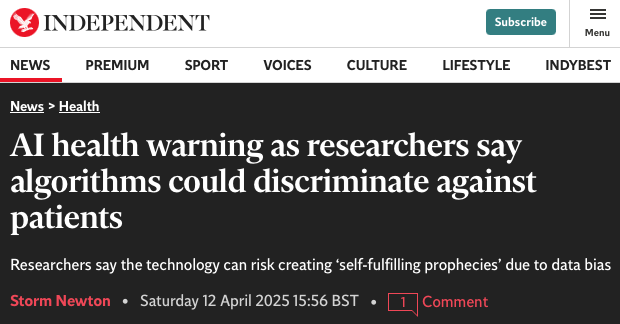
Press coverage
Science Media Center Roundup (7 experts)
Deterministic evaluation of usefulness of policy