A causal viewpoint on prediction model performance under changes in case-mix
Methods meeting at the Julius Center, UMC Utrecht
2024-11-25
Change in setting
What can we expect from the model’s performance (if anything) in the new setting?

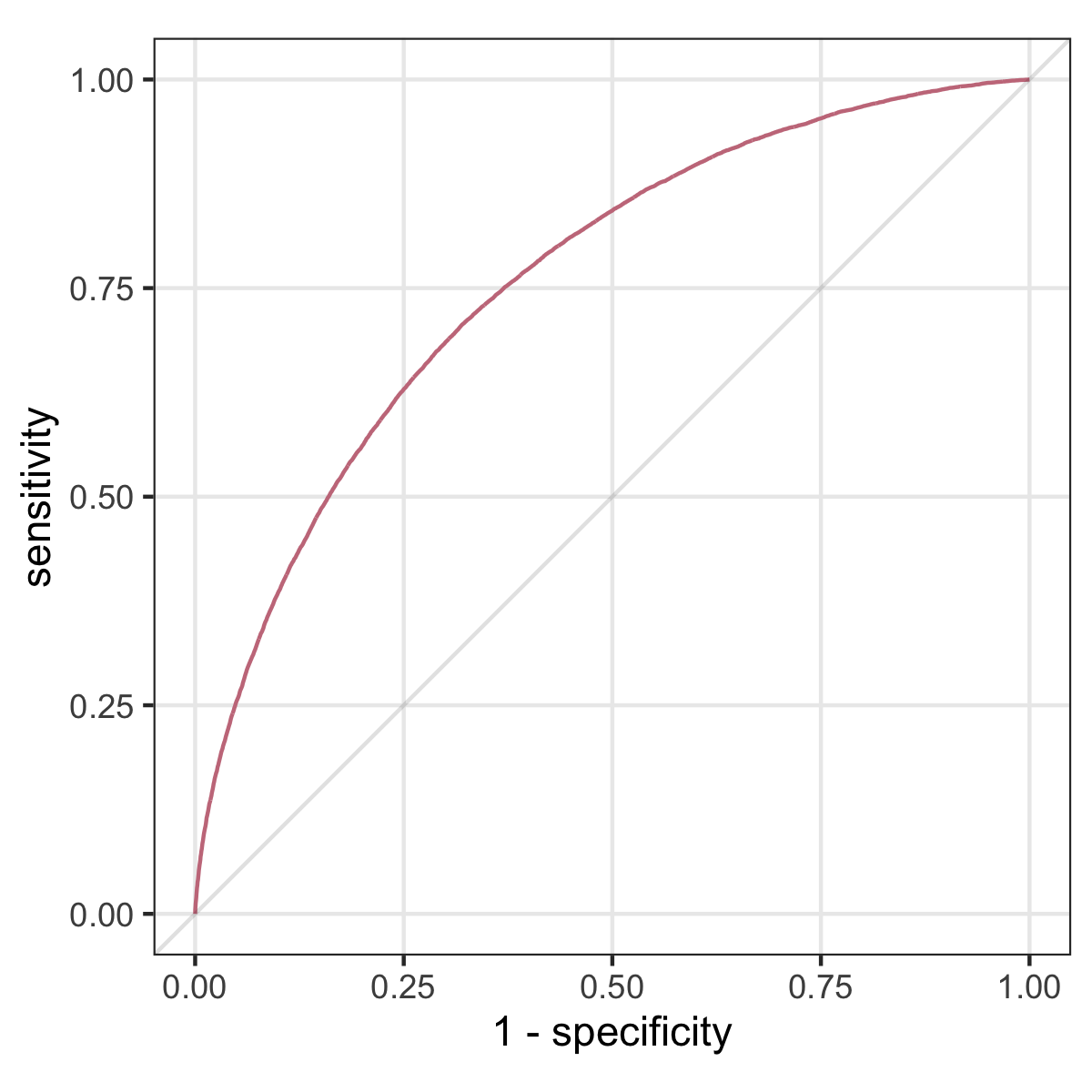
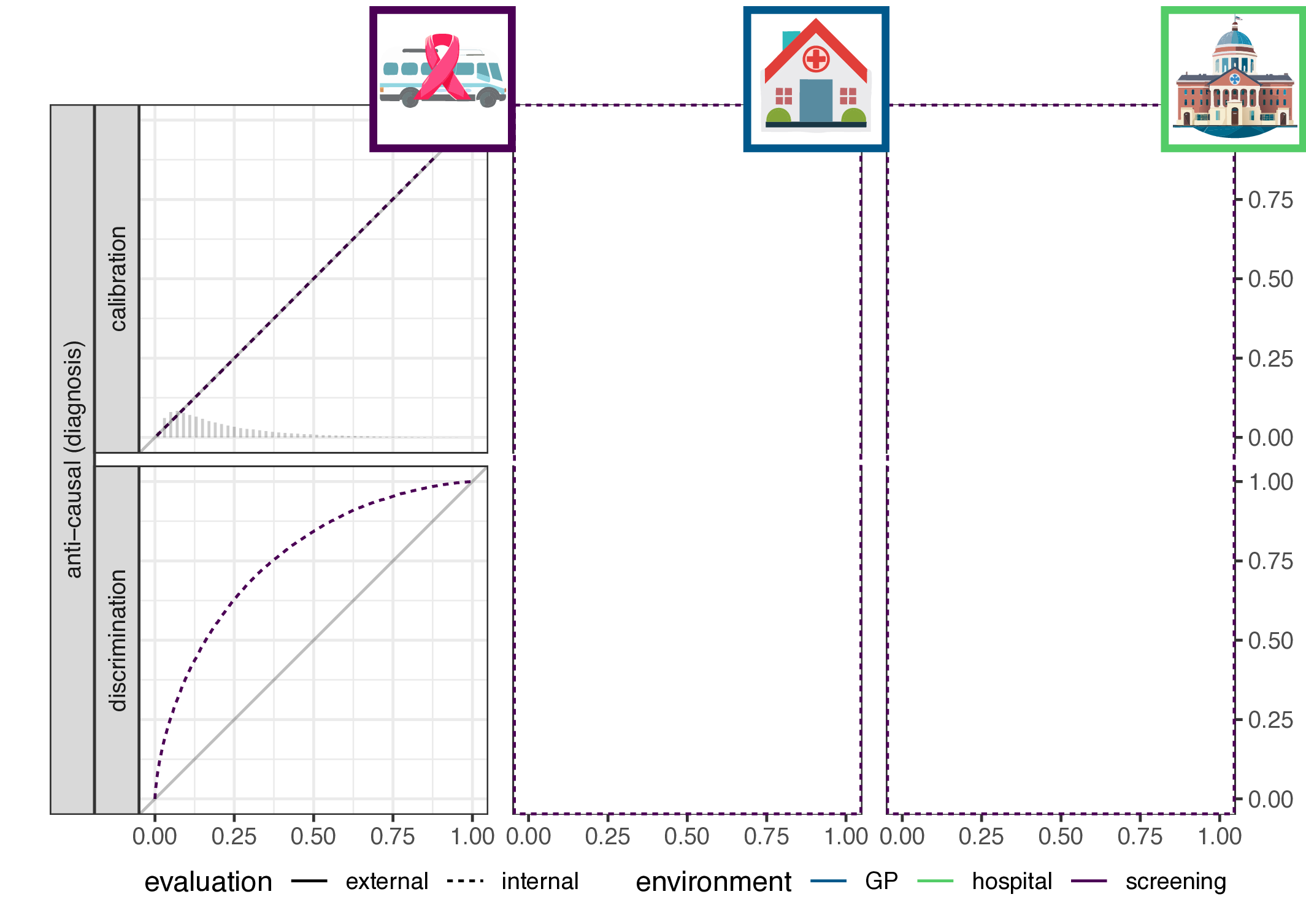
Discrimination: ROC curve and AUC
if we vary the threshold \(0 \leq \tau \leq 1\), we get a ROC curve, and the AUC is the area under this curve
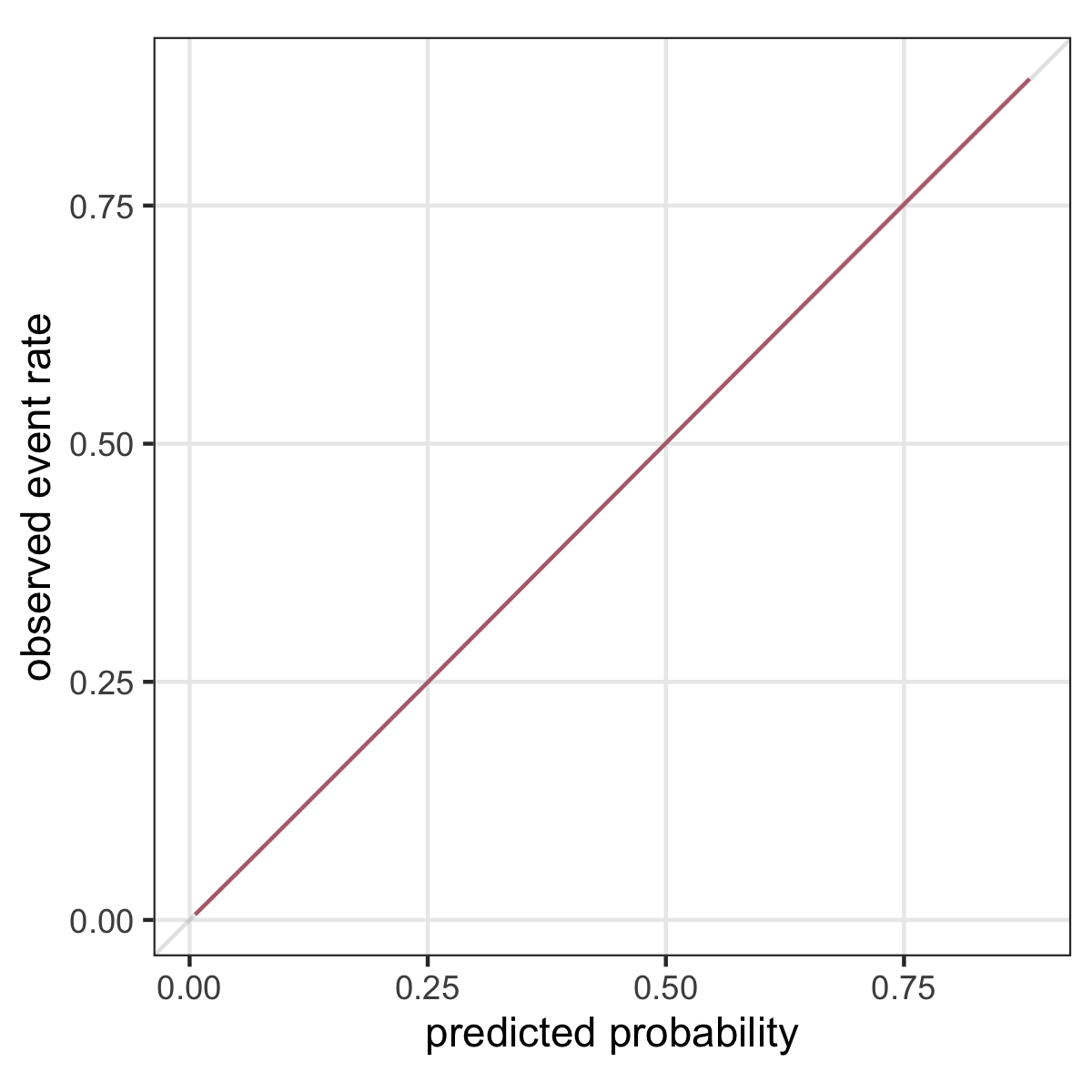
Calibration
“A model is said to be well calibrated if for every 100 patients given a risk of x%, close to x have the event.” (Van Calster and Vickers 2015)



Calibration plot
\(p(Y=1|X)\) versus \(f(x)\)

Where does the association come from?
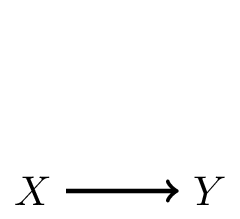
In prediction, we have features \(X\) and outcome \(Y\) and model \(Y|X\)
1. \(X\) causes \(Y\): often in prognosis (\(Y\): heart-attack, \(X\): cholesterol and age)
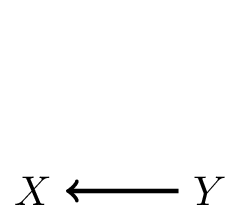
2. \(Y\) causes \(X\): often in diagnosis (CVA, based on neurological symptoms)
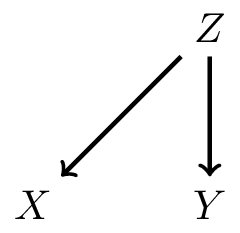
3. \(Z\) causes both \(X\) and \(Y\): confounding (yellow fingers predict lung cancer)
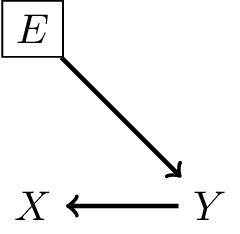
Defining a shift in case-mix
Define a shift in case-mix a change in the marginal distribution of the cause variable, e.g.
- filter on risk factors (pregancies with type 1 diabetes in hospital)
- filter on outcome risk (send patients with neurological symptoms to CVA center)
- denote environment as variable \(E\):

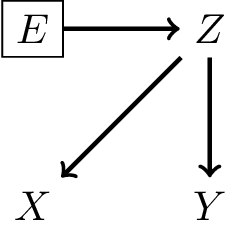
What does this definition imply?
- \(P(Y|X,E) = P(Y|X)\)
- in words: \(P(Y|X)\) is transportable across environments
- because there is no arrow from \(E\) to \(Y\), \(X\) blocks effect of \(E\) on \(Y\)
- \(P(X|Y,E) \neq P(X|Y)\)
- in words: \(P(X|Y)\) is not transportable across environments
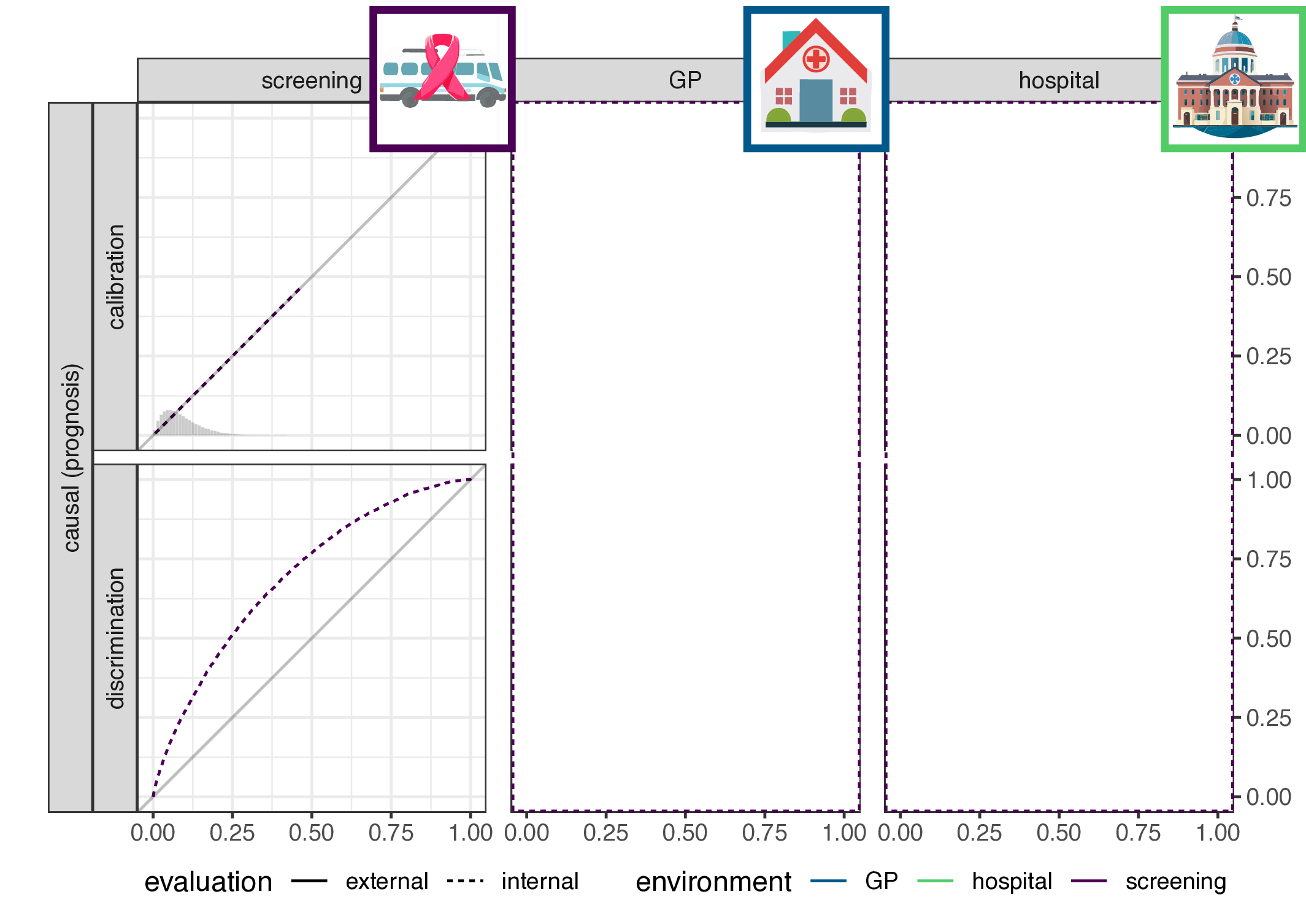
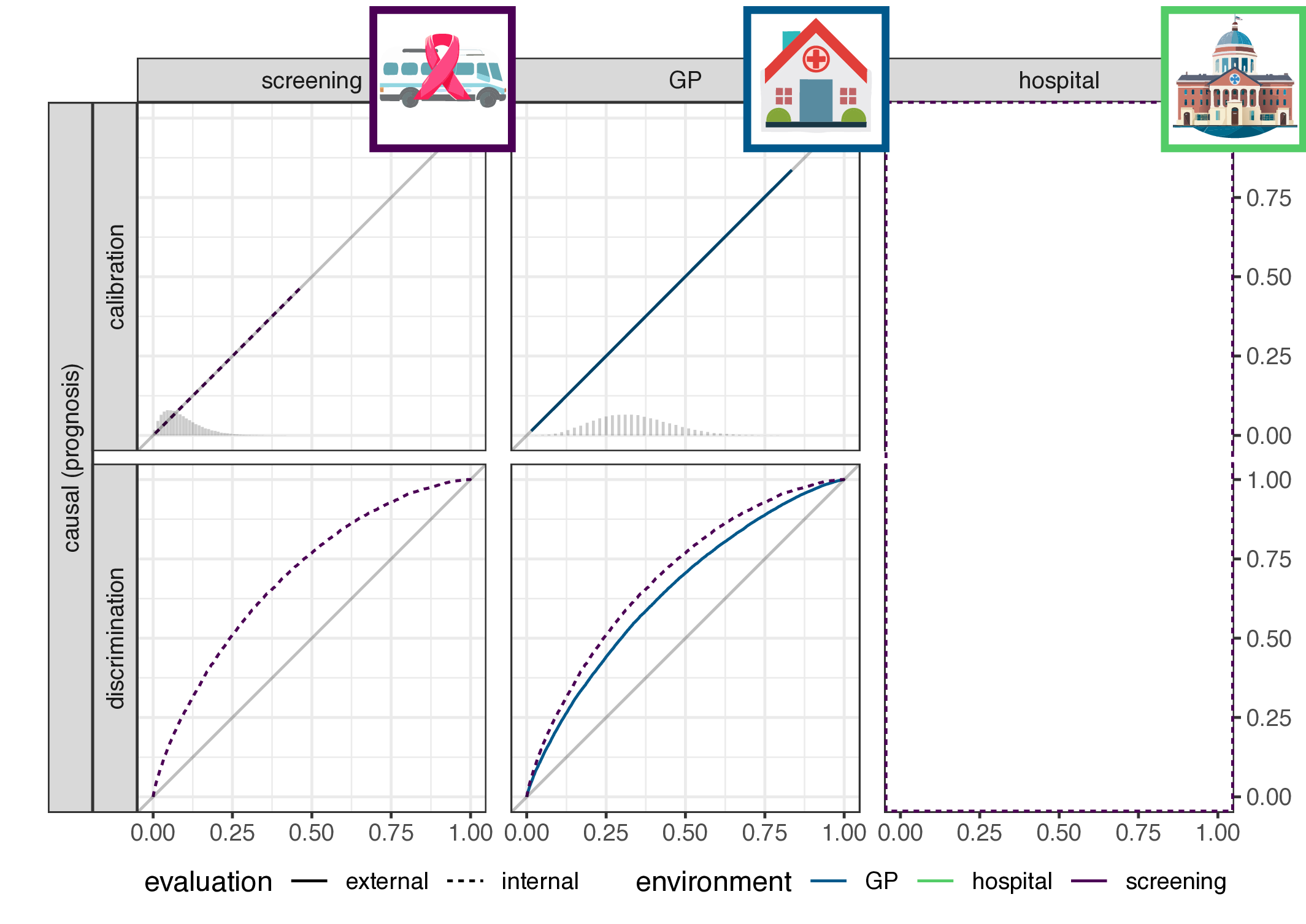
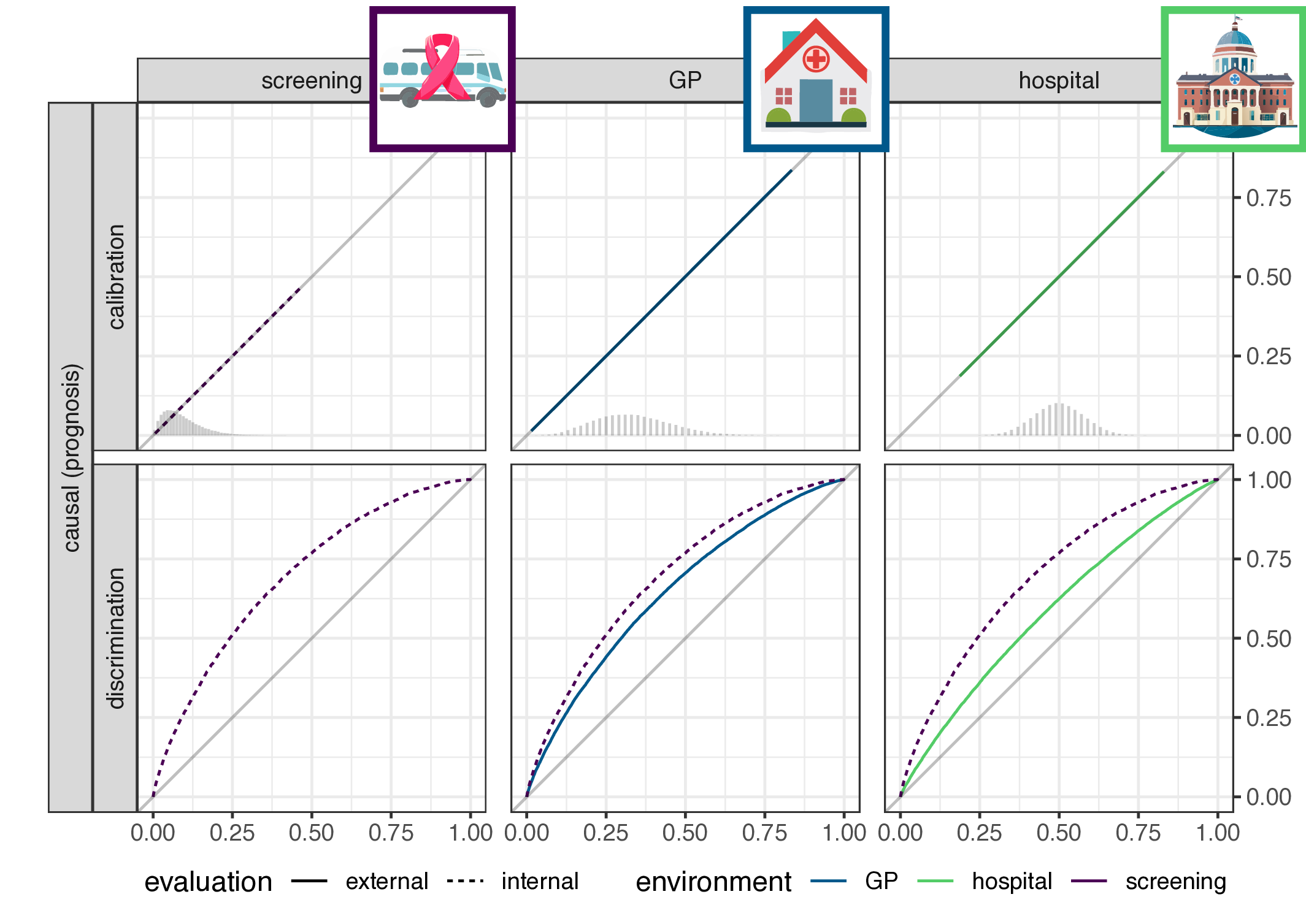
- implication for causal (prognosis) prediction:
- calibration is functional of \(P(Y|X)\), thus stable
- discrimination is functional of \(P(X|Y)\), thus not stable
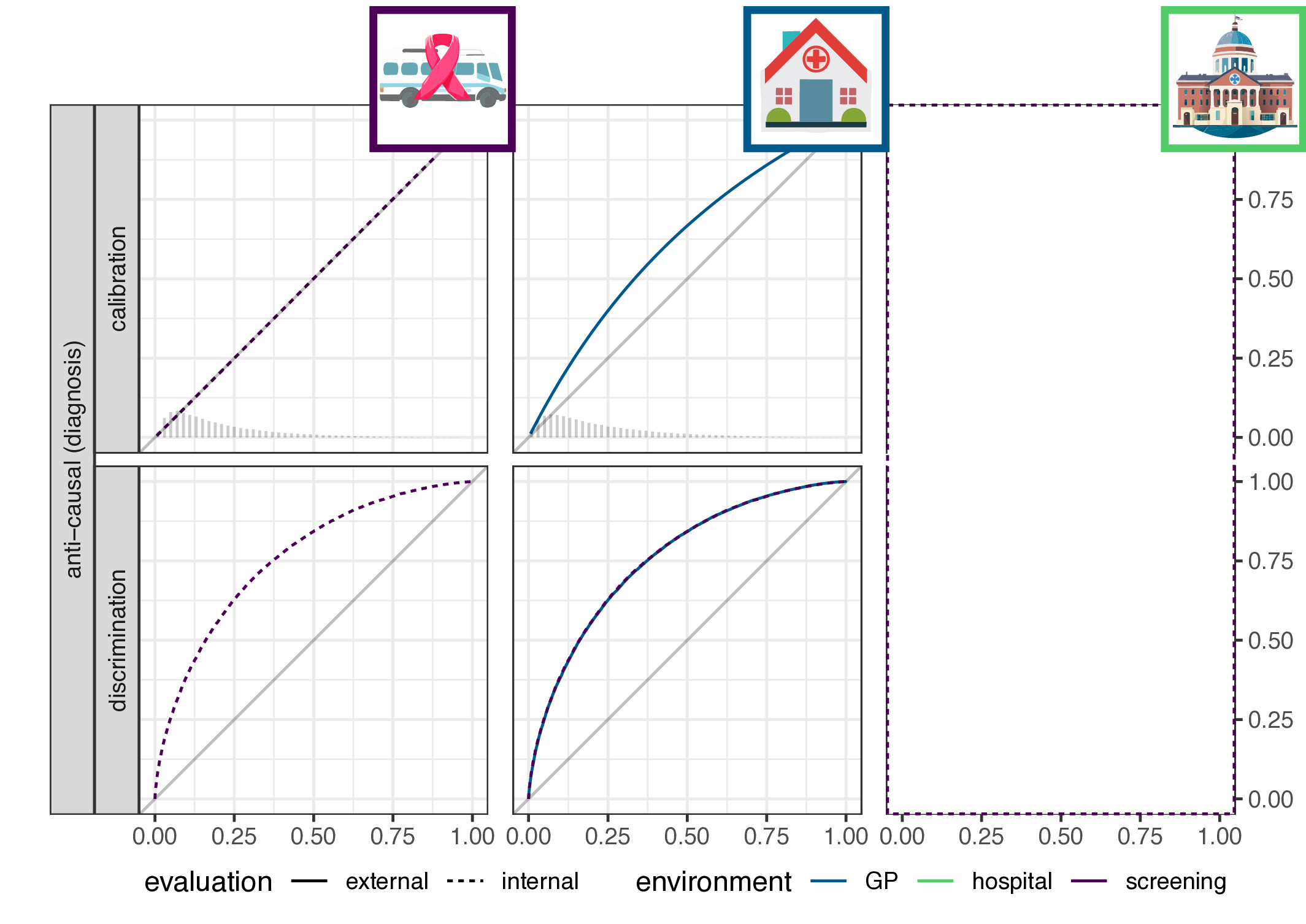
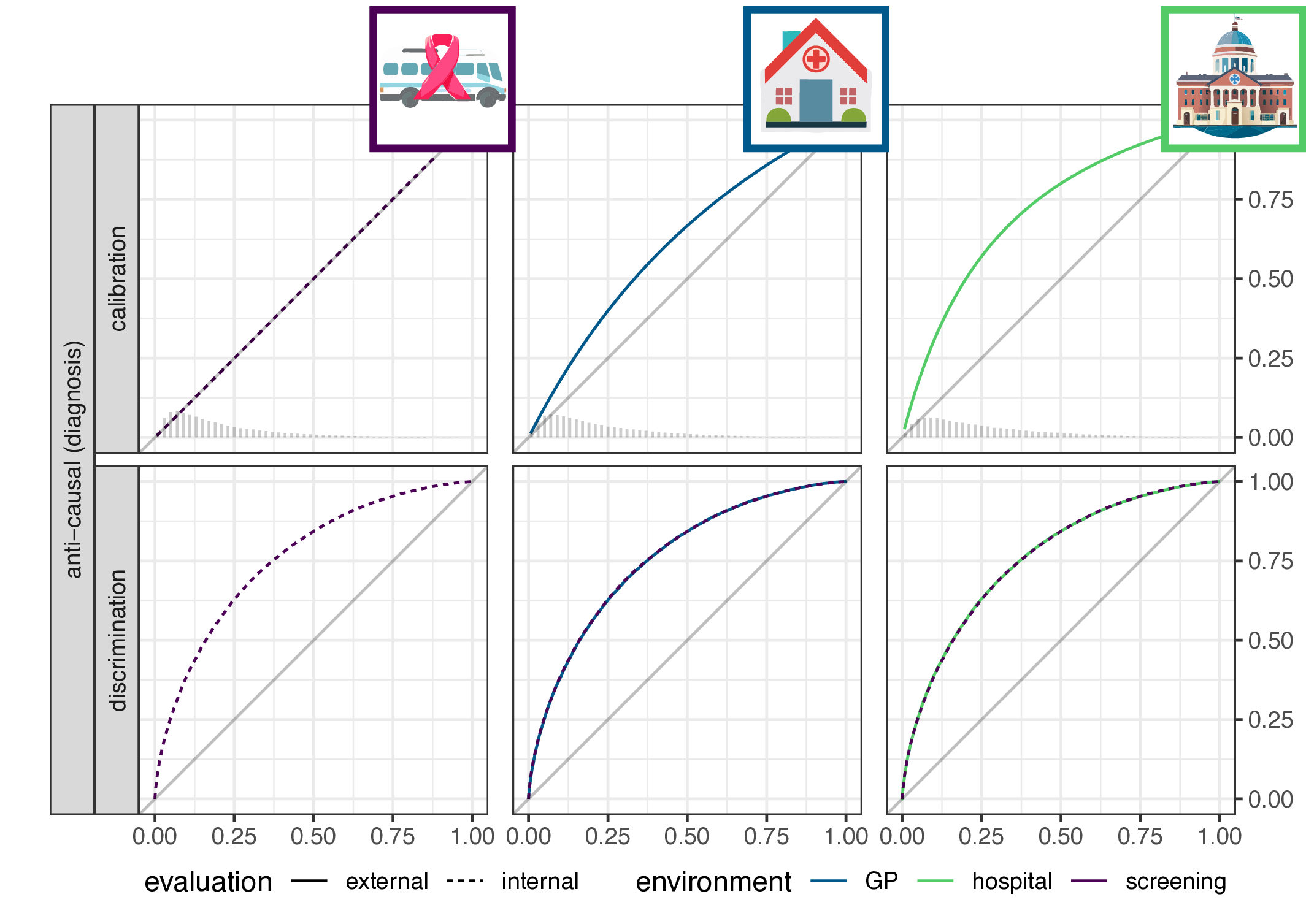
- for anti-causal (diagnosis) prediction: the reverse
- main result: discrimination or calibration may be preserved under changes in case-mix, but never both
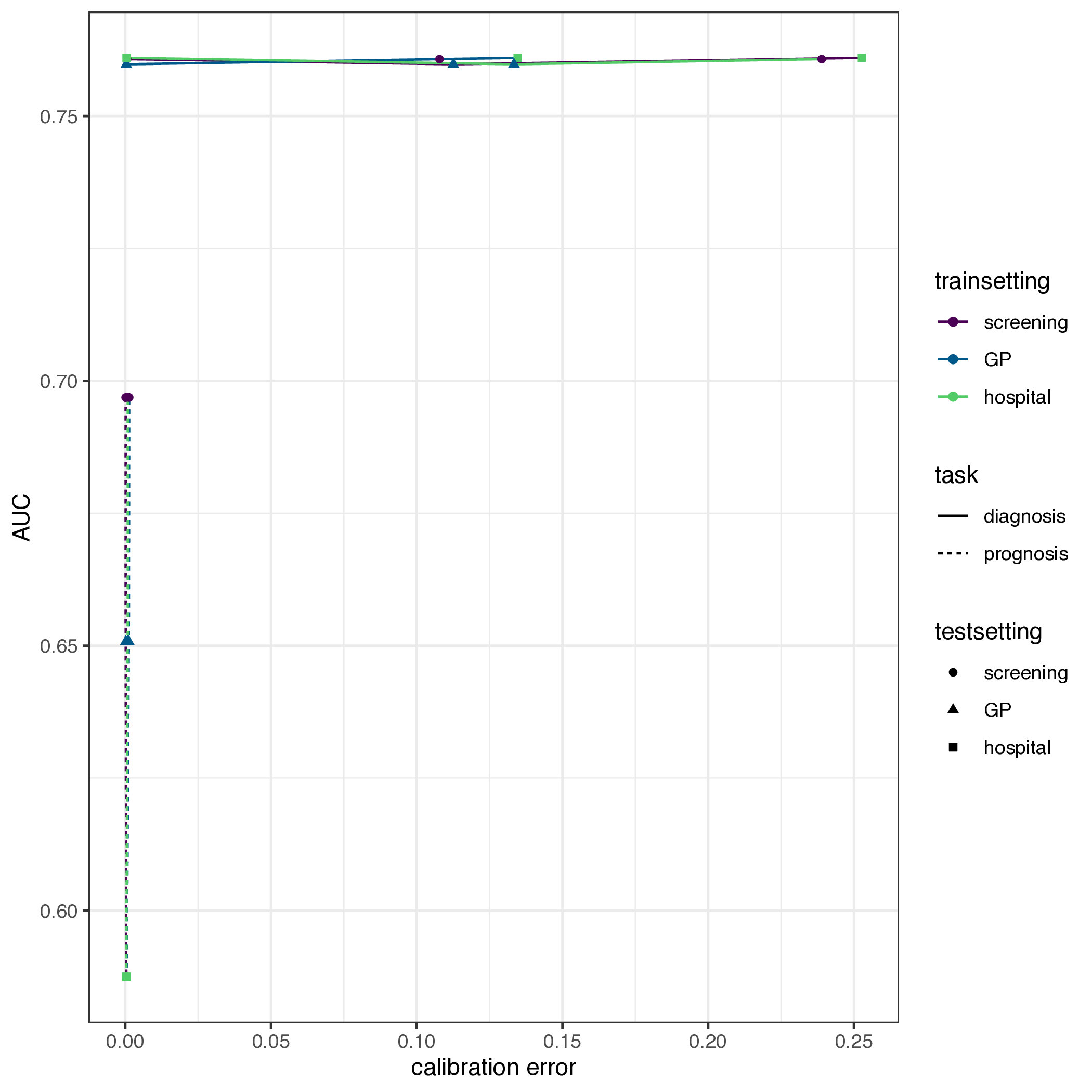
Empirical validation
- a study of 2030+ evaluations of 1300+ prediction models (Wessler et al. 2021)

- registry: all data available with only 4000 clicks
- solution: scrape the website