Pearl Causal Hierarchy
Causal Inference at Julius reading group
2024-11-06
The ladder is a hierarchy of questions
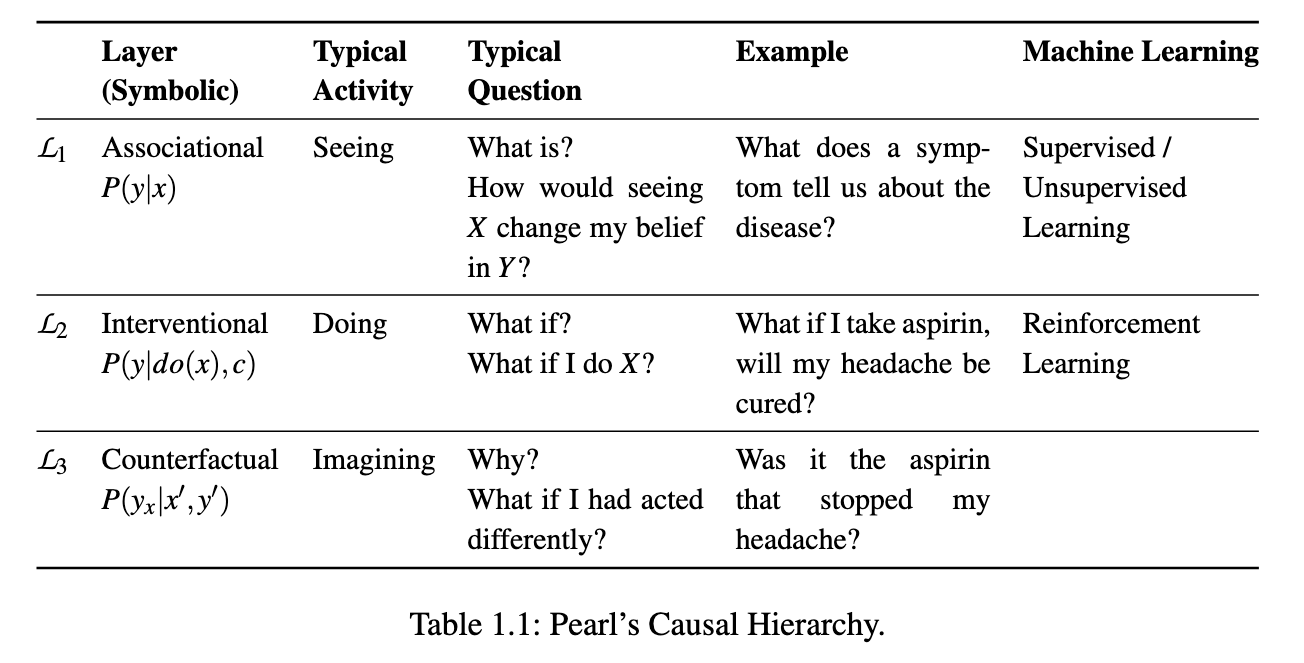
table 1
Layer 2: intervention, what is required?
- data where \(X\) is controlled by experimentation (randomized controlled trial)
- observational data + sufficient assumptions, typically:
- the directed acyclic graph (DAG) for the variables and no unobserved confounders
What is a SCM?

definition of SCM
- \(U\) is a set of background variables, also called exogenous variables, that are determined by factors outside the model;
- \(V\) is a set \(\{V_1,V_2,...,V_n\}\) of variables, called endogenous, that are determined by other variables in the model - that is, variables in \(U\cup V\);
- \(F\) is a set of functions \(\{ f_1, f_2,..., f_n\}\) such that each fiis a mapping from (the respective domains of) \(U_i \cup Pa_i \to V_i\), where \(U_i \subset U\), \(Pa_i \subset V - Vi\), and the entire set \(F\) forms a mapping from \(U\) to \(V\). That is, for \(i = 1,...,n\), each \(f_i \in F\) is such that
\[v_i \leftarrow f_i(pa_i, u_i)\]
- i.e., it assigns a value to \(V_i\) that depends on (the values of) a select set of variables in \(U \cup V\); and
- \(P(U)\) is a probability function defined over the domain of \(U\).
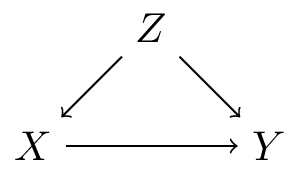
How are SCMs and DAGs related?
A recursive SCM implies a DAG, by following the order of arguments in the set of functions \(F\). E.G.:
\[ F = \begin{cases} Z \leftarrow f(U_Z) \end{cases} \]
How are SCMs and DAGs related?
A recursive SCM implies a DAG, by following the order of arguments in the set of functions \(F\). E.G.:
\[ F = \begin{cases} Z \leftarrow f(U_Z) \\ X \leftarrow f(Z, U_X) \end{cases} \]
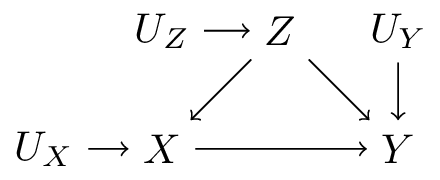
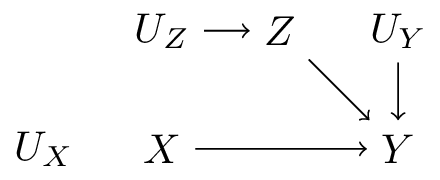
How are SCMs and DAGs related?
A recursive SCM implies a DAG, by following the order of arguments in the set of functions \(F\). E.G.:
\[ F = \begin{cases} Z \leftarrow f(U_Z) \\ X \leftarrow f(Z, U_X) \\ Y \leftarrow f(X, Z, U_Y) \end{cases} \]
Intervening in a SCM: a submodel
A recursive SCM implies a DAG, by following the order of arguments in the set of functions \(F\). E.G.:
\[ F = \begin{cases} Z \leftarrow f(U_Z) \\ X \leftarrow X' \\ Y \leftarrow f(X, Z, U_Y) \end{cases} \]
We can compute the effect of an action by replacing one \(f\) with a constant, e.g. \(X \leftarrow X'\), keep everything else the same, and evaluate the outcomes
Theorem 1
Theorem 1
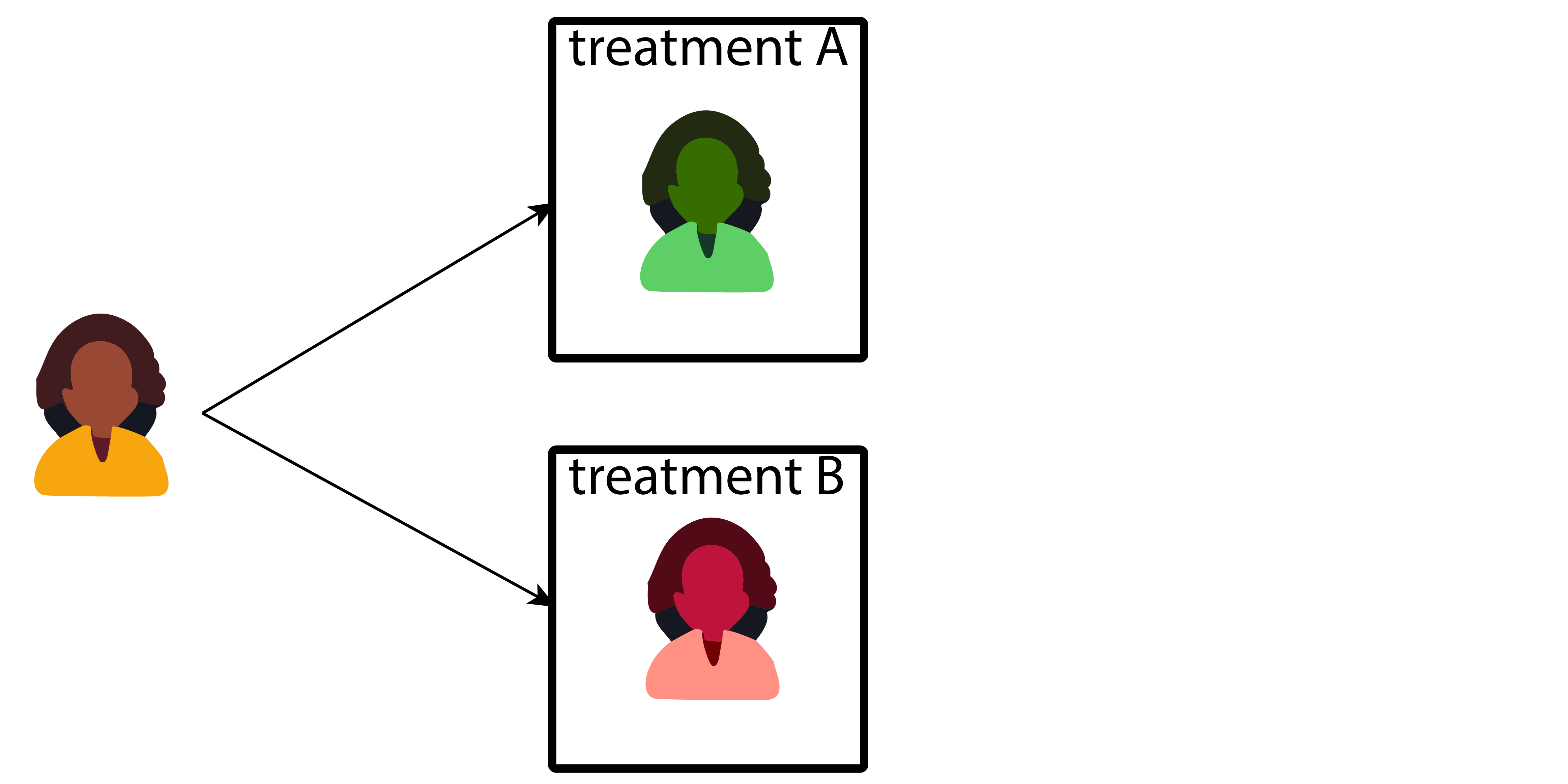
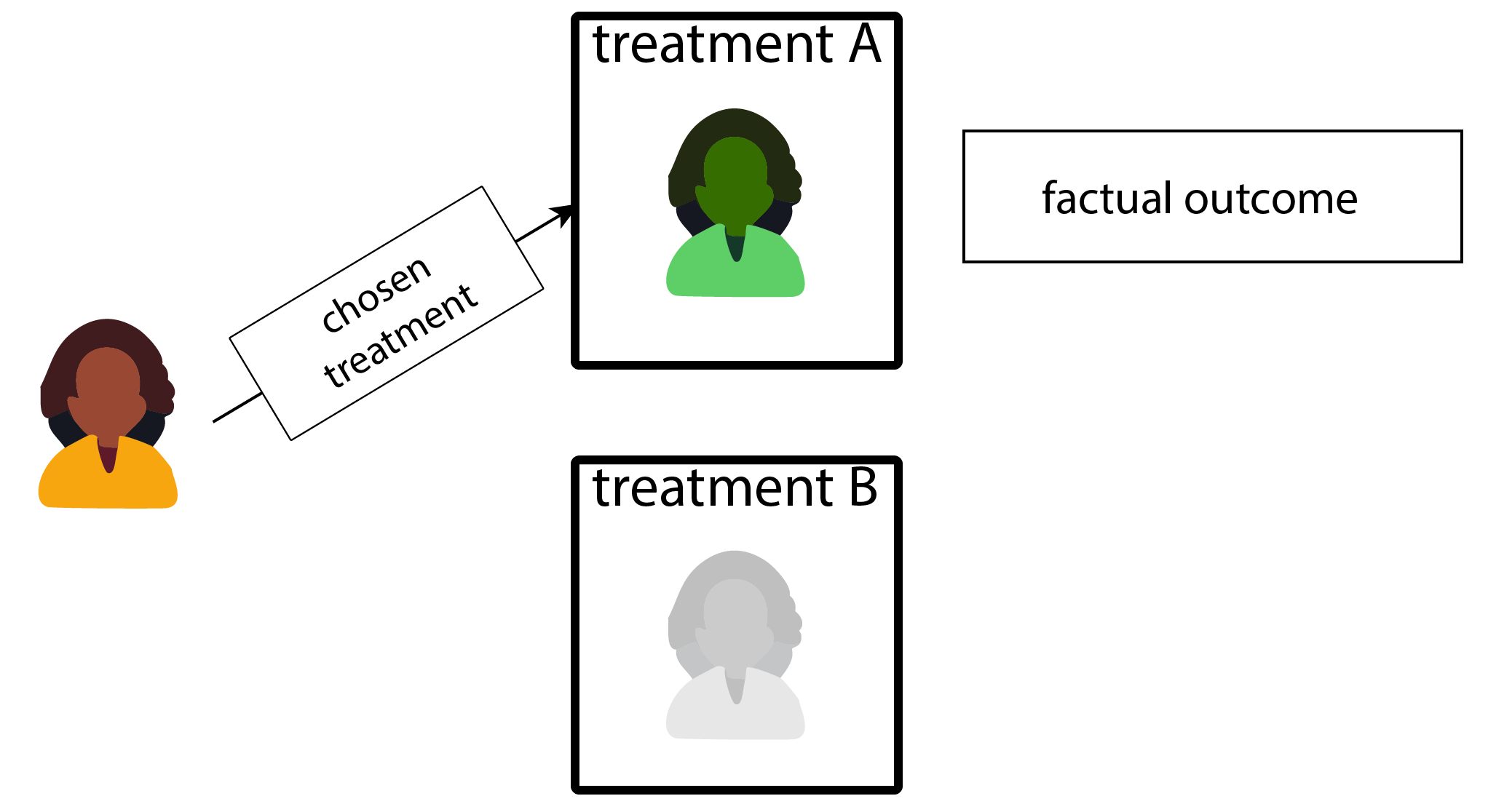
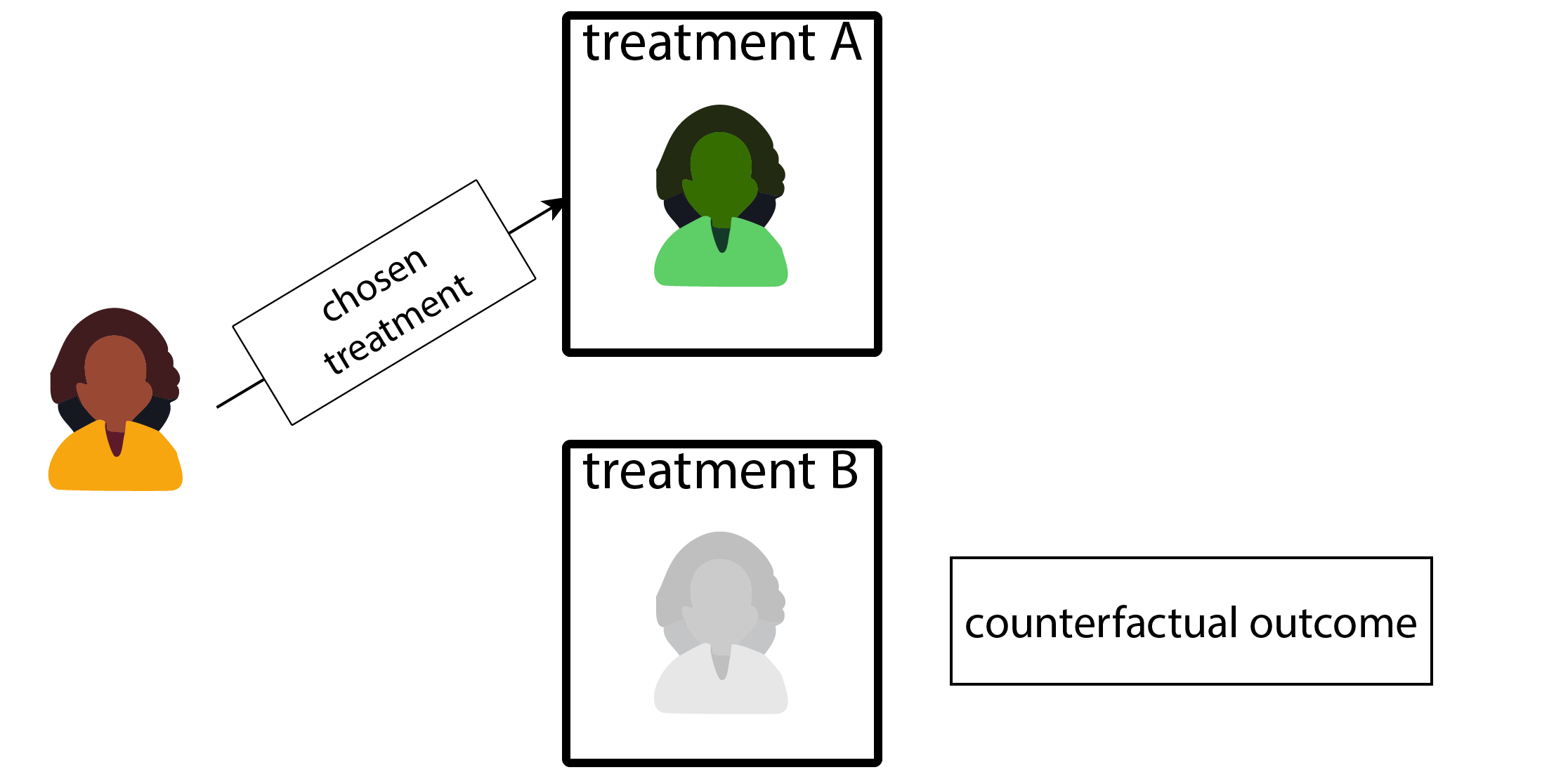
Potential outcomes framwork:
Image two possible futures for a patient